
Translate this page into:
5-hydroxyindole acetic acid level in cerebrospinal fluid as a potential biological marker for suicide
 , Jayanthi Yadav1,, Arneet Arora1, Abhijit Rozatkar2, Ajay Shukla3, Rishabh Chandela1, Sangita Moirangthem1
, Jayanthi Yadav1,, Arneet Arora1, Abhijit Rozatkar2, Ajay Shukla3, Rishabh Chandela1, Sangita Moirangthem1
*Corresponding author: Jayanthi Yadav, Department of Forensic Medicine and Toxicology, All India Institute of Medical Sciences, Bhopal, Madhya Pradesh, India. jayanthi.fmt@aiimsbhopal.edu.in
-
Received: ,
Accepted: ,
How to cite this article: Bhushan D, Yadav J, Arora A, Rozatkar A, Shukla A, Chandela R, et al. 5-hydroxyindole acetic acid level in cerebrospinal fluid as a potential biological marker for suicide. J Lab Physicians. doi: 10.25259/JLP_328_2024
Abstract
Objectives:
This study aimed to investigate the potential use of cerebrospinal fluid (CSF) 5-hydroxyindole acetic acid (5-HIAA) as a biomarker for suicidal behavior.
Materials and Methods:
Seventy-one autopsy cases were included in the study, of which 35 were classified as suicidal cases and 36 as non-suicidal cases. The median 5-HIAA level in the CSF was measured and compared between the two groups. Receiver operating characteristic (ROC) curve analysis was used to establish the diagnostic accuracy and optimal CSF 5-HIAA cutoff levels for discriminating suicide from non-suicide.
Statistical analysis:
The statistical analyses involved t-tests, Mann-Whitney, chi-square, and Fisher exact tests as appropriate. ROC curves assessed the diagnostic value of CSF-5-HIAA, and the p-values less than 0.05 were considered statistically significant.
Results:
The ROC analysis revealed a threshold value of 87.64 nMol/L for 5-HIAA, with a sensitivity of 54% and specificity of 86%. The median CSF 5-HIAA level was significantly lower in suicidal cases compared to non-suicidal cases (86.27 nMol/L vs. 107.06 nMol/L, P = 0.001).
Conclusions:
The study suggests that CSF 5-HIAA may be a potential biomarker for identifying suicidal behavior. This finding could contribute to developing more effective prevention and treatment strategies for suicide and suicidal behavior.
Keywords
5-hydroxyindole acetic acid
Cerebrospinal fluid
Forensic medicine
Serotonin
Suicide

INTRODUCTION
Suicide and suicidal behavior are significant public health issues that continue to impact individuals and communities worldwide. In India, suicide is a significant public health issue, with the national suicide rate of 12.[1] Identifying reliable biological markers for these complex phenomena could help improve prevention and treatment strategies. One potential biological marker studied in this context is the 5-hydroxyindole acetic acid (5-HIAA) level in the cerebrospinal fluid (CSF).[2]
Serotonin is a neurotransmitter that plays a role in regulating mood, emotion, and behavior. 5-HIAA is a metabolite of Serotonin, and studies have shown that individuals who have died by suicide or who have attempted suicide have lower levels of 5-HIAA in their CSF.[3,4] CSF 5-HIAA remains stable when stored at −80°C and has also been observed to maintain stability for up to 48 h at room temperature.[5] In contrast to 5-Hydroxytryptamine (5-HT), 5-HIAA is known to be stable in postmortem samples, not sensitive to plastic consumables, and requires no addition of chemicals like ascorbic acid to prevent degradation.[5-7] Acetaminophen increases brain serotonin levels by inhibiting hepatic tryptophan 2,3-dioxygenase.[8] CSF 5-HIAA levels are also decreased by desipramine and zimeldine.[9] Dialysis has been shown to decrease CSF levels of 5-HIAA.[10] Strenuous exercise may raise 5-HIAA levels.[11] Spearman’s correlation did not show significant associations between CSF 5-HIAA levels in different genders of any age group.[12] The normal level of CSF 5-HIAA was 93.3 ± 33.6 nMol/L.[13]
To investigate the potential of CSF 5-HIAA levels in suicide, we conducted an observational study of 71 autopsy cases at a tertiary care hospital in India. We measured CSF 5-HIAA levels using Ultraviolet (UV)-high-performance liquid chromatography (HPLC) and compared levels in suicidal and non-suicidal cases. We also used receiver operating characteristic (ROC) curve analysis to establish optimal cutoff levels for discriminating between suicide from non-suicide.
MATERIALS AND METHODS
Autopsy instruments, syringe with needle, Eppendorf tubes, centrifugation machine, Acrodisc sterile syringe filter having a pore size of 0.22 µm and 25 mm diameter (Pall Corporation, United States), compatible freezer (−80°C), 5-Hydroxyindole-3-acetic acid (Merck/sigma), acetonitrile (Sigma-Aldrich, United States), concentrated formic acid, concentrated acetic acid, methanol, phosphoric acid, ultrafilter (Ultra 370 series RIONS INDIA), electronic balance machine, 1000 mL measuring cylinder, micropipettes and HPLC (Waters 2489 UV/Visible detector).
The Institutional Human Ethics Committee approved this study for our institute’s Post-graduate Research vide letter of permission letter no 2020/PG/Jan/09 dated November 21, 2020. The sampling method was convenient sampling and included all the medico-legal cases that arrived at the Mortuary of our institute for autopsy from November 2020 to May 2022, fulfilling the inclusion and exclusion criteria. The inclusion criteria were all suicidal cases in which clear CSF was obtained during the autopsy, and for control, all non-suicidal cases in which clear CSF was obtained during the autopsy were taken, and exclusion criteria included relatives not willing to give consent, decomposed bodies, head injury cases, and any case in which clear CSF was not found. A total of 71 cases were taken, including 35 suicidal (24 males and 11 females) and 36 non-suicidal (25 males and 11 females) cases as controls. All samples were collected within 24 h (6–24 h) of death to reduce variability and potential confounding factors associated with postmortem changes. The cases were selected as case/control based on the alleged history given by relatives or police before starting the autopsy, and later manner of death confirmed by police investigations and autopsy findings.
Once it was established that the deceased body fulfilled the inclusion and exclusion criteria, the next of kin and a family member were fully informed about the study, along with a printed participant information sheet, and after having the written consent form filled and duly signed by the next of kin, the CSF was collected. The history of each subject regarding the use of specific medications, drugs, and certain foods known to influence the measured concentration of 5-HIAA was taken to rule out any potential alterations in the CSF 5-HIAA levels. By accounting for these potential confounders, the research aimed to better understand the relationship between CSF 5-HIAA levels and suicidality.
During the autopsy, after opening the skull and removal of the dura, a sterile needle with a 10 mL syringe attached to it was inserted into the dependent and posterior part of the lateral ventricle of the brain for around 1.5 cm depth. The needle was directed posteriorly and downwards in the ventricle, and CSF was aspirated. About 4–5 mL of CSF was collected from the brain’s lateral ventricles. Then, the CSF was transferred to the 5 mL Eppendorf tubes. The CSF was centrifuged upon collection at 15,000 rpm for 15 min at 4°C and filtered with a sterile nylon syringe filter with a pore size of 0.22 µm. The CSF sample was stored at −80°C freezer until analysis.
UV-HPLC analysis to detect the 5-HIAA in CSF samples was carried out blindly at the Department of Biological Sciences, Indian Institute of Science Education and Research, Bhopal. The 5-HIAA in CSF samples was resolved by the HPLC pump system (Waters 515) fitted with Waters 2489 UV/Visible Detector and reverse phase SunFireTM C-18 column, 5 µm, 4.6 × 25 mm. The mobile phase containing formic acid (0.05%) and acetonitrile in 1:9 at a flow rate of 1.0 mL/min, determined at 280 nm were found to be optimum to resolve the peak of 5-HIAA with a running time of 20 min; these parameters obtained were further used to analyze all the clinical samples.[14] The concentration of 5-HIAA in each clinical sample was determined using the standard solution of 100 nM 5-HIAA (Merck, India). All the runs were carried out in triplicate to check the repeatability of the results. We calculated the CSF 5-HIAA concentration from a UV-HPLC analysis quantitatively by comparing it with the standard sample concentration . A comparison of the area under the curve for the unknown sample (cases) and that of the known sample was used to determine the amount of CSF 5-HIAA in samples.
Statistical analysis
The data obtained from the analysis was entered into Microsoft Excel and analyzed using R Studio version 4.2.0. The statistical analyses involved t-tests, Mann–Whitney, Chi-square, and Fisher’s exact tests as appropriate. ROC curves assessed the diagnostic value of CSF-5-HIAA, and P < 0.05 was considered statistically significant.
RESULTS
Out of the total of 71 cases, 35 were suicides, while 36 were non-suicidal. The suicidal cases included 24 cases with hanging and 11 cases of poisoning as a cause of death. Out of non-suicidal cases, the cause of death varied from road traffic accidents and homicides (without head injury) to sudden deaths, for example, myocardial infarction, pancreatitis, and others. The age-wise distribution of cases is mentioned [Table 1].
| Age (in years) | No. of suicidal cases (%) | No. of non-suicidal cases (%) | Total no. of cases (%) |
|---|---|---|---|
| <18 years | 2 (6) | 1 (3) | 3 (4) |
| 19–30 years | 15 (43) | 8 (22) | 23 (32) |
| 31–40 years | 13 (36) | 8 (22) | 21 (30) |
| 41–50 years | 2 (6) | 9 (25) | 11 (16) |
| 51–60 years | 2 (6) | 5 (14) | 7 (10) |
| >60 years | 1 (3) | 5 (14) | 6 (8) |
| Total | 35 (100) | 36 (100) | 71 (100) |
The median level of 5-HIAA in CSF was significantly lower in suicidal cases (86.27 nMol/L) compared to non-suicidal cases (107.06 nMol/L), with P= 0.001. The interquartile range for suicidal cases was 72.39–105.10 nMol/L, and for non-suicidal cases was 93.55–124.26 nMol/L. The ROC curve analysis established a threshold value of 87.64 nMol/L for discriminating suicide from non-suicide with a sensitivity of 54% and specificity of 86% [Figure 1].
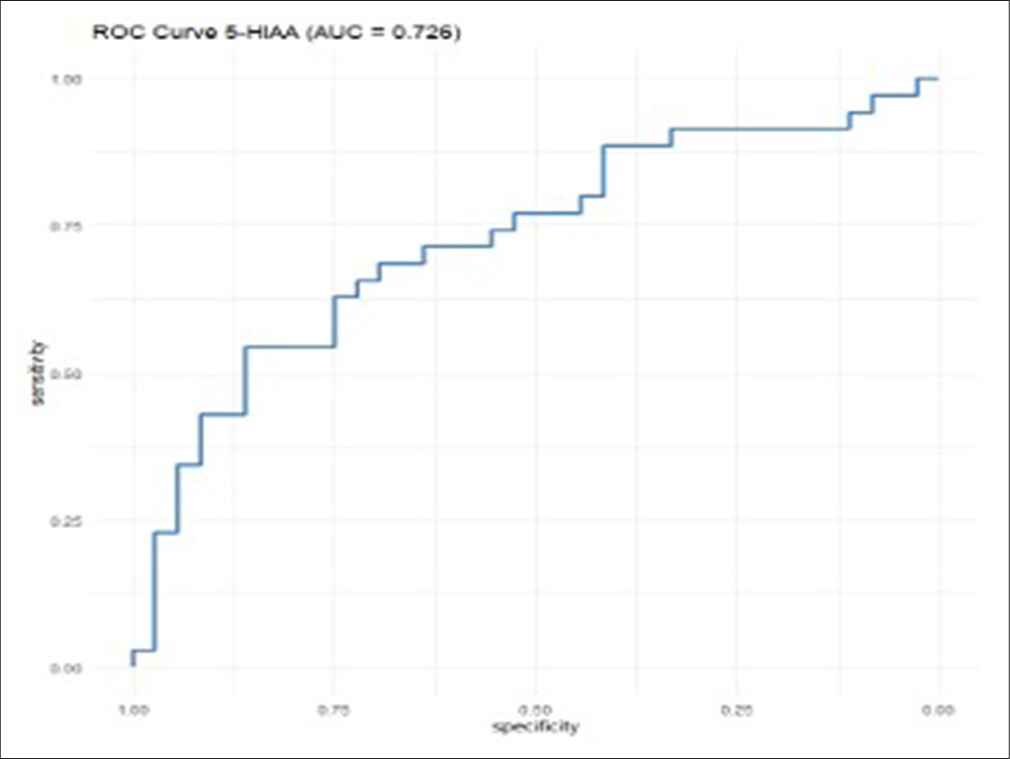
- 5-HIAA receiver operating characteristic curve (Area under the curve = 0.726) for prediction of suicide. 5-HIAA: 5-hydroxyindole acetic acid, ROC: Receiver Operating Characteristic, AUC: Area Under the Curve.
For predicting suicide in suicidal behavior cases, the ROC curve analysis established a threshold value of 85.87 nMol/L with a sensitivity of 84% and specificity of 72% [Figure 2]. A value lower than the cutoff of 85.87 nMol/L in suicidal behavior cases is suggestive of the autopsy case being a suicide, as compared to values higher than the cutoff. The study shows that the 5-HIAA level in CSF could potentially serve as a biomarker for predicting suicide, especially in cases of suicidal behavior.
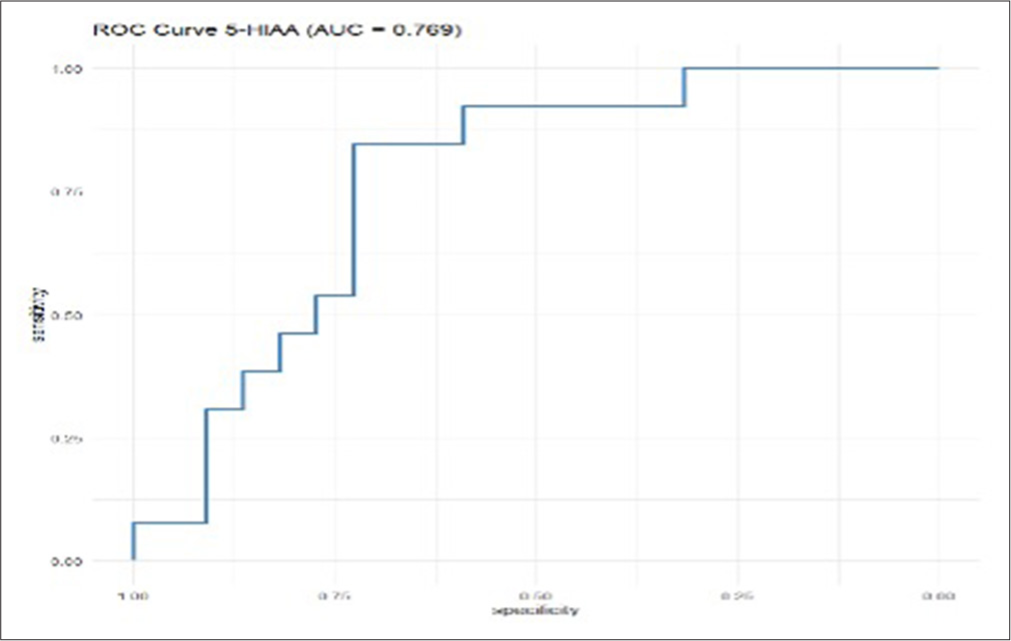
- 5-HIAA receiver operating characteristic curve (Area under the curve = 0.769) for prediction of suicide in past suicidal behavior cases. 5-HIAA: 5-hydroxyindole acetic acid, ROC: Receiver Operating Characteristic, AUC: Area Under the Curve.
DISCUSSION
Serotonin is a neurotransmitter that regulates several physiological processes, including mood, appetite, sleep, and pain. Serotonin is synthesized from the amino acid tryptophan through enzymatic reactions in the brain and other tissues. Serotonin exerts its effects by binding to specific receptor subtypes throughout the body.
After Serotonin is released into the synaptic cleft, it can be taken up by the presynaptic neuron through a specific transporter protein called the serotonin transporter, which terminates its action. Inside the pre-synaptic neuron, Serotonin can be metabolized by the enzyme monoamine oxidase into 5-hydroxyindoleacetaldehyde (5-HIAA), which is then further metabolized into 5-hydroxyindoleacetic acid (5-HIAA). Measurement of the levels of 5-HIAA in the CSF has been used as an indirect indicator of serotonin activity in the brain. Decreased levels of 5-HIAA in the CSF have been associated with several mental health disorders.[15,16]
CSF 5-HIAA has been studied as a potential biomarker for suicide and suicidal behavior for several decades. Studies have suggested that low levels of 5-HIAA in the CSF may be associated with an increased risk of suicide and suicidal behavior.[17] One of the early studies investigating the relationship between 5-HIAA and suicidal behavior was conducted in the 1980s. The study found that patients who had attempted suicide had lower levels of 5-HIAA in their CSF compared to patients with other psychiatric disorders and healthy controls.[18] Several subsequent studies have supported these findings, and some have also suggested that low 5-HIAA levels may be a trait marker for suicidal behavior.[19,20] Interestingly, we found similar results as a significant difference in CSF 5-HIAA levels between suicidal and non-suicidal cases, with the median level being significantly lower in suicidal cases (86.27 nMol/L) than in non-suicidal cases (107.06 nMol/L).
To determine the diagnostic accuracy and optimal CSF 5-HIAA cutoff levels for discriminating suicide from non-suicide, ROC curve analysis was performed. The threshold value of 5-HIAA was found to be 87.64 nMol/L, with a sensitivity of 54% and specificity of 86%. In addition to these findings, the study also examined the predictive value of CSF 5-HIAA levels for suicidal behavior in suicidal behavior cases. ROC curve analysis demonstrated an optimal cutoff value of 85.87 nMol/L, with a sensitivity of 84% and specificity of 72%.
In the autopsy setting, measurement of 5-HIAA levels in the CSF can provide important information for understanding the pathophysiology of mental health disorders, including those that are associated with suicide. Measuring 5-HIAA levels in the CSF can also be used to assess the efficacy of pharmacological treatments that affect the serotonergic system in the brain. In the clinical setting, the measurement of 5-HIAA levels in the CSF can be used to aid in the diagnosis of specific mental health disorders, such as major depression and bipolar disorder. In addition, CSF 5-HIAA levels may help predict the response to specific antidepressant treatments, as well as identify individuals who may be at increased risk for suicidal behavior.
Several limitations of the current research on 5-HIAA levels as a biological marker for suicide and suicidal behavior have been identified. These include the impact of confounding factors and the small sample sizes in some studies. Overall, this study highlights the potential utility of CSF 5-HIAA levels as a biomarker for identifying individuals at risk of suicide. However, it is essential to note that 5-HIAA levels can be influenced by various factors, such as age, gender, medication use, and comorbid psychiatric disorders.[21] However, further research is needed to validate these findings and determine the clinical utility of this biomarker in a larger population of at-risk individuals.
CONCLUSIONS
Our manuscript sheds light on the potential of 5-HIAA as a marker for determining suicide in medico-legal cases, offering valuable insights into the manner of death. We have demonstrated its significance as a reliable indicator in postmortem investigations through meticulous analysis and correlation with other forensic evidence.
Furthermore, the implications extend beyond autopsy settings. Our findings suggest the promising prospect of utilizing 5-HIAA levels in living patients as a means of early detection of suicidal behavior. By integrating this biomarker into clinical assessments, healthcare professionals may gain a valuable tool for identifying at-risk individuals and intervening before tragedy strikes.
Looking ahead, the application of 5-HIAA in suicide prevention holds immense potential. With further research and validation, this biomarker could revolutionize psychiatric care by enabling timely interventions and tailored support for those vulnerable to suicidal ideation and behaviors. Ultimately, our manuscript underscores the urgent need for continued exploration of biomarkers like 5-HIAA to advance suicide prevention strategies and save lives. In addition, more comprehensive studies can examine the efficacy of integrating 5-HIAA with other clinical and psychological markers for suicide risk assessment. This may lead to more accurate risk assessment and a more effective prevention strategy for suicide.
Acknowledgment:
The authors thank the Department of Forensic Medicine and Toxicology, AIIMS. Bhopal and ICMR for their support, and the deceased for their silent cooperation.
Author contribution:
JY: Conceptualisation, establishing methodology and guidance; DB: Carrying out the study and acquiring grant, manuscript compilation; AA: Guidance and facilitation; AR: Guidance in analysing suicidal cases; AS: Guidance in laboratory analysis of HIAA; RC: Manuscript writing and editing; SM: Manuscript writing and editing.
Ethical approval:
The research/study was approved by the Institutional Review Board at All India Institute of Medical Sciences, Bhopal, number 2020/PG/Jan/09, dated 21st November 2020.
Declaration of patient consent:
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest:
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation:
The authors confirm that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship: Indian Council of Medical Research MD/MS Thesis Financial Support.
References
- The psychological autopsy: An overview of its utility and methodology. J Neurosci Rural Pract. 2023;14:447-52.
- [CrossRef] [PubMed] [Google Scholar]
- Suicide prevention strategies: A systematic review. JAMA. 2005;294:2064-74.
- [CrossRef] [PubMed] [Google Scholar]
- Higher expression of serotonin 5-HT (2A) receptors in the postmortem brains of teenage suicide victims. Am J Psychiatry. 2002;159:419-29.
- [CrossRef] [PubMed] [Google Scholar]
- CSF 5-HIAA predicts suicide risk after attempted suicide. Suicide Life Threat Behav. 1994;24:1-9.
- [CrossRef] [PubMed] [Google Scholar]
- Stability of monoamine metabolites in human cerebrospinal fluid. Ann Neurol. 1982;12:48-51.
- [CrossRef] [PubMed] [Google Scholar]
- Correlations between aminergic metabolites simultaneously obtained from human CSF and brain. Life Sci. 1985;37:1279-86.
- [CrossRef] [PubMed] [Google Scholar]
- Serotonin concentrations and turnover in brains of depressed suicides. Brain Res. 1989;502:332-40.
- [CrossRef] [PubMed] [Google Scholar]
- Exercise and sleep in aging: Emphasis on serotonin. Pathol Biol (Paris). 2014;62:276-83.
- [CrossRef] [PubMed] [Google Scholar]
- Acetaminophen inhibits liver trytophan-2,3-dioxygenase activity with a concomitant rise in brain serotonin levels and a reduction in urinary 5-hydroxyindole acetic acid. Life Sci. 2000;67:235-40.
- [CrossRef] [PubMed] [Google Scholar]
- Selective antidepressants and cerebrospinal fluid. Lack of specificity on norepinephrine and serotonin metabolites. Arch Gen Psychiatry. 1985;42:1171-7.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of dialysis on plasma and CSF tryptophan and CSF 5-hydroxyindoleacetic acid in advanced renal disease. J Neurol Neurosurg Psychiatry. 1980;43:739-43.
- [CrossRef] [PubMed] [Google Scholar]
- Cerebrospinal fluid levels of 5-hydroxyindoleacetic acid in Parkinson's disease and atypical Parkinsonian syndromes. Neurodegener Dis. 2021;21:30-5.
- [CrossRef] [PubMed] [Google Scholar]
- Elevated cerebrospinal fluid 5-hydroxyindoleacetic acid levels in women with comorbid depression and panic disorder. Int J Neuropsychopharmacol. 2006;9:547-56.
- [CrossRef] [PubMed] [Google Scholar]
- Validated ultraviolet high-performance liquid chromatography method for post-mortem 5-hydroxy-indoleacetic acid measurement in human cerebrospinal fluid. J Lab Physicians. 2023;16:58-64.
- [CrossRef] [Google Scholar]
- Candidate endophenotypes for genetic studies of suicidal behavior. Biol Psychiatry. 2009;65:556-63.
- [CrossRef] [PubMed] [Google Scholar]
- Antidepressants increase neural progenitor cells in the human hippocampus. Neuropsychopharmacology. 2009;34:376-2389.
- [CrossRef] [PubMed] [Google Scholar]
- 5-HIAA in the cerebrospinal fluid. A biochemical suicide predictor? Arch Gen Psychiatry 1976. ;. ;33:1193-97.
- [CrossRef] [PubMed] [Google Scholar]
- Serotonin 1A receptors, serotonin transporter binding and serotonin transporter mRNA expression in the brainstem of depressed suicide victims. Neuropsychopharmacology. 2003;28:359-66.
- [Google Scholar]
- CSF monoamine metabolites in melancholia. Acta Psychiatr Scand. 1984;69:201-19.
- [CrossRef] [PubMed] [Google Scholar]
- Monoamine transporters and the psychopharmacology of suicide. Ann New York Acad Sci. 2000;836:120-39.
- [Google Scholar]



