
Translate this page into:
Evaluation of Tear Film Urea Level as a Diagnostic Marker of Dry Eye Disease: A Pilot Study
 , Anil Sharma2, Hitender S. Batra3, Subrahmanya Murti Velamakanni4, Mansur Khan5, Sandeep Gupta6
, Anil Sharma2, Hitender S. Batra3, Subrahmanya Murti Velamakanni4, Mansur Khan5, Sandeep Gupta6
Address for correspondence: Gurunadh Satyanarayana Velamakanni, MS, DO, Department of Ophthalmology, GSL Medical College, Lakshmipuram, Rajahmundry, Andhra Pradesh 533296, India (e-mail: subrahmanyamurti@yahoo.co.in).
This article was originally published by Thieme Medical and Scientific Publishers Pvt. Ltd. and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Introduction
Urea secreted in the sweat is important for skin moisture. Similarly, ocular surface moisture is maintained by the conjunctiva. Based on this, the level of urea in tear film can be used as a potential diagnostic test for dry eye disease (DED). One of the standard tests for DED is Schirmer's test (ST). The aim of this study was to compare tear film urea to values of ST.
Methods
Fifty patients symptomatic for DED having ST ≤ 10 mm/5 min were enrolled in the study. Fifty age- and sex-matched asymptomatic subjects with ST>10 mm/5 min were taken as controls. All patients were subjected to an estimation of tear film urea, collected using micropipettes, and analyzed by an Erba Chem 5 semi-autoanalyzer. Based on the ST reading as per the Dry Eye Workshop 2007 (DEWS) classification, dry eye was classified as dry eye (≤ 10 mm/5 min), severe dry eye (≤ 5 mm/5 min), and very severe dry eye (≤ 2 mm/5 min). Tear film urea values were compared with ST values that were considered standard. Statistical analysis was done using Medcalc version 19.7. A p-value ≤ 0.05 was considered significant.
Results
The mean tear film urea levels in cases were (26.78±5.70 mg/dL) significantly lower compared with controls (41.72±6.86 mg/dL). The area under the receiver characteristic operator curve (AUC) for tear film urea in diagnosing DED was 0.936 (p<0.0001) with a cutoff of ≤ 37.2 mg/dL, yielding a sensitivity of 96% and a specificity of 76%. For diagnosing severe DED, the AUC for tear film urea was 0.824 (p<0.0001) with a cutoff value of ≤ 23.4 mg/dL, yielding a sensitivity of 60.8% and a specificity of 92.59%. For diagnosis of very severe DED, the AUC for tear film urea was 0.972 (p<0.0001) with a cutoff value of ≤ 19.8 mg/dL, yielding a sensitivity of 100% and a specificity of 93.62%. On comparing ST values to tear film urea, the regression coefficient was 0.85 (p<0.0001), suggesting a linear relationship between ST and tear film urea.
Conclusion
The study demonstrates that tear film urea can be a potential diagnostic marker for DED. The study also indicates that tear film urea level is linearly related to Schirmer's test values and provides an approximate diagnostic cutoff level for the design of future large-scale studies.
Keywords
dry eye disease
Schirmer's test
tear film urea

Introduction
One of the morbidities seen in general ophthalmic practice is the dry eye disease (DED). It is also a fact that the incidence of this entity is increasing by the day. In an assessment among a large claims database in the US, DED that was ranked fifth among reasons for presenting for ophthalmic examination in 2008 jumped to third place by 2012.[1] Over a 10-year period, in the Beaver Dam Study, the incidence of dry eye symptoms in the subjects was 21.6%.[2] Despite the increasing morbidity of DED, this is one entity in ocular practice where there are no definitive laid down directives from the criteria of diagnosis to the agent of choice for treatment. This aspect has also led to an increase in the research into the various aspects of DED.
A common function of skin and conjunctiva is that both these structures attempt to keep their surfaces moist. The sebaceous and the sweat glands are involved in keeping the skin surface from drying, whereas there are the lacrimal glands for the ocular surface. The lacrimal fluid, which is aqueous, constitutes 90% of the tear volume. There exists, therefore, an analogy between the conjunctiva and the skin. However, there is no analogy with regard to treatment strategies. In dermatology practice, various moisturizers have no application in ophthalmology. However, one ingredient in use in dermatology as a moisturizer is urea. Urea is an important hygroscopic component of the epidermis, and as a part of the natural moisturizing factor of the skin, it helps in the maintenance of skin hydration. Consequently, the reduced hygroscopic potential of dry skin leads to trans-epidermal loss of water. There is also an aberrant expression of genes encoding epidermal structural and catalytic proteins. The role of urea in hydrating the skin has now included the regulation of epidermal genes necessary for proper barrier function.[3] In this background, the study by Jäger et al[4] has shown that the ocular surface has a well-coordinated system of enzymes that produce urea, and in DED the concentration of urea is reduced. It needs to be emphasized at this juncture that topical moisturizing agents are the cornerstone of the treatment of dry skin conditions and since long, urea-containing formulations have been used in various concentrations to moisturize the skin.
These observations would lead to reasoning that evaluation of urea concentration in the tear fluid may throw light into the complex issue of DED and when the same be compared with Schirmer's test (ST), the most common evaluator of DED, an understanding into this common ocular morbidity can be achieved.
A study was thereby performed to estimate the levels of urea in the tear fluid and compare the same to ST values among the patients attending the outpatient department (OPD) of an ophthalmic unit of a tertiary care hospital. The study was started after taking a written, informed consent following careful selection of study subjects as per the inclusion and exclusion criteria and after obtaining clearance from the institute ethics committee.
Disclosure
The same data sample as used for this study with only descriptive statistics has been published by Sharma et al previously.[5] This work represents the complete regression analysis of the data sample comparing tear film urea levels to values of ST.
Materials and Methods
A prospective, observational, single-center, matched case–control study was conducted at a tertiary care eye center. Consecutive sampling was used. Patients attending eye OPD who were having symptoms suggestive of dry eyes were considered for enrolment in the study as cases. These were foreign body sensation, ocular dryness, grittiness, redness, mucoid discharge, ocular irritation, excessive tearing (secondary to reflex secretion), photophobia, and fluctuating or blurry vision. Patients attending eye OPD without the above complaints constituted the control population. Controls were chosen after appropriate matching.
These cases were then subjected to ophthalmic examination consisting of assessment of best-corrected visual acuity, slit-lamp biomicroscopic examination of the cornea, anterior chamber (AC), lens and anterior vitreous followed by fundus examination with direct ophthalmoscopy and with slit-lamp using 90D. The intraocular pressure (IOP) was measured with Goldman's applanation tonometer. Cycloplegic refraction was performed, if required.
Selected patients were then called for ST on a different day. The testing was done as per the standard procedure.[6] Patients having wetting ≤ 10 mm at 5 minutes were considered as having dry eyes and 50 such patients were enrolled in the study as cases. Schirmer's test was also conducted on age- and sex-matched patients who did not complain of any of the symptoms elaborated above. Among these, 50 subjects having wetting more than 10 mm at 5 minutes and with age and sex matching the study population were enrolled in the study as controls.
Exclusion criteria: Patients with a history of any previous ocular surgery were excluded. Patients with any medical comorbidities and kidney disease, particularly, were excluded from the study.
All enrolled patients were then subjected to the assessment of urea levels in the tear fluid. Based on the ST reading, DED was classified as dry eye (≤ 10 mm/5 min), severe dry eye (≤ 5 mm/5 min), and very severe dry eye (≤ 2 mm/5 min) as per the Dry Eye Workshop 2007 classification.[7] These values were then analyzed with respective tear film urea levels and an attempt was made to assess the value of tear urea levels compared with ST as the diagnostic gold standard. Tear film samples were collected my micropipettes and analyzed using the Erba Chem 5 semi-autoanalyzer (Erba Diagnostics, Manheim, Germany).
Statistical analysis was done using Medcalc version 19.7 (Medcalc software Inc, Ostend, Belgium). A p-value ≤ 0.05 was considered significant.
Results
The demographics and the urea levels in the tears and serum have already been published.[5] As it was a matched case–control study, there was no significant difference between cases and controls. The mean age of the study population was 42.88±17.8 years with a male to female ratio of 1.17:1. There were no significant differences between tear urea levels between males and females. The mean tear film urea levels in the cases with dry eye (26.78±5.70 mg/dL) were significantly lower compared with those of controls (41.72±6.86 mg/dL) (►Table 1). On regression analysis comparing ST values to tear film urea, the coefficient was 0.85 with a p<0.0001, suggesting a linear relationship between ST and tear film urea (►Fig. 1). On further regression analysis, there was no significant connection between age and levels of ST (r=0.04, p=0.66), suggesting that ST values do not reduce with increasing age.
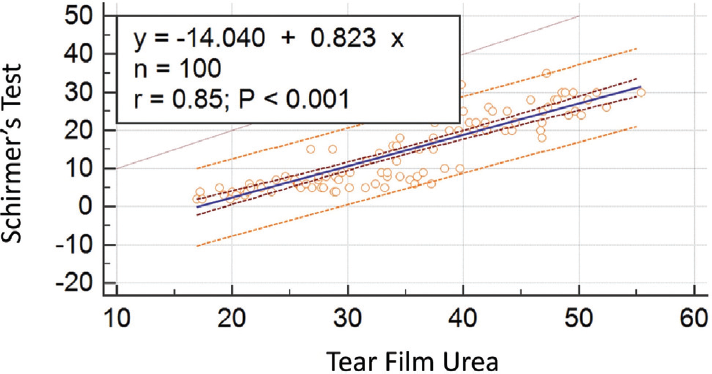
- Scatter plot of linear regression comparison of tear film urea levels with Schirmer's test values showing a regression coefficient of 0.85, implying a linear relationship between the two variables.
| Parameter | Cases (n=50) | Controls (n=50) | p-Value | |
|---|---|---|---|---|
| Mean age (y) | 42.83±17.63 | 42.8269±17.29 | 0.99 | |
| Male to female ratio | 0.78:1 | 0.85:1 | 0.42 | |
| Mean blood urea (mg/dL) | 38.36±8.73 | 38.39±7.98 | 0.99 | |
| Mean tear film urea (mg/dL) | Total | 26.78±5.70 | 41.72±6.86 | < 0.001 |
| Females | 27.06±5.27 | 41.10±7.48 | < 0.001 | |
| Males | 27.53±7.11 | 42.43±6.58 | < 0.001 | |
| Median Schirmer's test value (mm/5 min) | 6 | 23 | < 0.001 | |
| Mean Schirmer's test value (mm/5 min) | 5.94±2.13 | 22.86±5.59 | < 0.001 | |
On receiver operator characteristic curve analysis (ROC) analysis for tear film urea in diagnosing DED (ST<10 mm/5 min), the area under the ROC curve (AUC) was 0.936 (p<0.0001) with a tear urea cutoff of ≤ 37.2 mg/dL, yielding a sensitivity of 96% and a specificity of 76%. Among those with DED, for diagnosing severe DED as against those without severe DED, for tear film urea, the AUC was 0.824 (p<0.0001). Further, for the diagnosis of very severe DED, the AUC for tear film urea was 0.972 (p<0.0001) (►Table 2).
| Tear film urea as a test for discriminating parameters | Area under ROC curve (AUC) | 95% Confidence Interval (CI) for AUC | p-Value for AUC | Youden cutoff Criterion (mg/dL) | Sensitivity (%) | Specificity (%) |
|---|---|---|---|---|---|---|
| Dry eye versus no dry eye | 0.936 | 0.869–0.975 | < 0.0001 | ≤ 37.2 | 96 | 76 |
| Severe dry Eye versus non severe dry eye | 0.824 | 0.691–0.917 | < 0.0001 | ≤ 23.4 | 60.87 | 92.59 |
| Very severe dry eye versus not very severe dry eye | 0.972 | 0.880–0.998 | < 0.0001 | ≤ 19.8 | 100 | 93.62 |
Discussion
In this study, when urea levels in the tear film of subjects with dry eye were compared with the same in normal individuals, there was a less value of urea in subjects, with the difference between the two being statistically significant. This finding corroborates with the study of Jäger et al[4] as brought out in the analysis.
There are various tests for the diagnosis of dry eye.[8] Large population-based studies have used different types of questionnaires, some self-administered and others by surveyors. National Eye Institute Visual Function Questionnaire-25 (NEI-VFQ25) and Ocular Surface Disease Index (OSDI)[9] are prominent among these questionnaires. Smaller studies have used objective tests.[10] The common among these have been ST and Tear-film Break up Time (TBUT). A few have used both subjective and objective tests. However, there is no gold standard test for the detection of DED.[11] It has been a common observation that among the questionnaires and the objective tests, the latter have detected lesser DED. Among TBUT and ST, the numbers of DED detected by ST have been less when compared with the numbers detected by TBUT. Based on this background, this study on the evaluation of tear film urea levels was based on ST.
This study has shown that urea levels are reduced in the tear fluid in eyes with DED. The regression analysis of tear film urea and ST showed a linear progression with an r=0.85 (p<0.001), inferring that the tear film urea decreases as Schirmer's wetting also decreases.
The areas under the receiver operator characteristic curves (AUC) for tear film urea for diagnosing DED were highly significant. The specificity of tear film urea levels with reference to DED based on ST was very high and more so in eyes with very severe dry eyes. This implies that when the wetting of the ST filter paper went down, so did the levels of urea in the tear fluid. The ROC analysis of tear film urea levels and ST however has not given good sensitivity. The findings of this study have brought forward the fact that tear fluid urea levels are reduced in eyes diagnosed as DED with ST.
Study Limitations
First, the sample size was small. Second, a matched case–controlled study design can have an inherent bias. The aim of the study is not to prove association or causality. It is merely a pilot evaluation to assess whether tear film urea levels can be used as a diagnostic marker for DED.
Conclusions
There is a constant effort by investigators and researchers to develop new strategies and drugs to improve the outcomes in dry eye syndromes. This study has added a new area of interest based on the urea levels in the tear fluid. The most important significant outcome of this study is the lower value of urea in the tear fluid in the eyes diagnosed with DED by ST as compared with controls. Because dry eye detection is the least when ST is taken for assessment, the results of this study assume significance. This reduction in the values of urea in the tear film is linearly associated with decreasing wetting of ST or in the other words increasing severity of DED. Our study is only a pilot analysis to determine the feasibility of studying tear film urea levels; in the future, larger and better planned studies are required. Further research on tear film urea as a diagnostic/prognostic marker for DED is kindled by the findings of this study.
Institutional Approval
This work received an institutional review and ethical approval from the ethics committee of the Armed Forces Medical College, Pune.
Conflicts of Interest
None declared.
References
- Long-term incidence of dry eye in an older population. Optom Vis Sci. 2008;85(08):668-674.
- [CrossRef] [PubMed] [Google Scholar]
- Dry eye disease ranking among common reasons for seeking eye care in a large US claims database. Clin Ophthalmol. 2019;13:225-232.
- [CrossRef] [PubMed] [Google Scholar]
- Urea: a clinically oriented overview from bench to bedside. J Drugs Dermatol. 2016;15(05):633-639.
- [Google Scholar]
- Enzymes of urea synthesis are expressed at the ocular surface, and decreased urea in the tear fluid is associated with dry-eye syndrome. Graefes Arch Clin Exp Ophthalmol. 2013;251(08):1995-2002.
- [CrossRef] [PubMed] [Google Scholar]
- Correlation between urea levels in lacrimal fluid and patho-physiology of dry eye syndromes. IOSR J Dent Med Sci. 2020;19:29-34.
- [CrossRef] [Google Scholar]
- The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop (2007) Ocul Surf. 2007;5(02):75-92.
- [CrossRef] [PubMed] [Google Scholar]
- Rasch analysis of the Ocular Surface Disease Index (OSDI) Invest Ophthalmol Vis Sci. 2011;52(12):8630-8635.
- [CrossRef] [PubMed] [Google Scholar]
- Short Tear Film Breakup Time-Type Dry Eye. Invest Ophthalmol Vis Sci. 2018;59(14):DES64-DES70.
- [CrossRef] [PubMed] [Google Scholar]
- Validation of an objective measure of dry eye severity. Transl Vis Sci Technol. 2018;7(05):26. DOI: 10.1167/tvst.7.5.26
- [CrossRef] [PubMed] [Google Scholar]



