
Translate this page into:
Sharma's Python Sign: A New Tubal Sign in Female Genital Tuberculosis
Address for correspondence: Dr. Jai Bhagwan Sharma, E-mail: jbsharma2000@gmail.com
This is an open access article distributed under the terms of the Creative Commons Attribution NonCommercial ShareAlike 3.0 License, which allows others to remix, tweak, and build upon the work non commercially, as long as the author is credited and the new creations are licensed under the identical terms.
This article was originally published by Medknow Publications & Media Pvt Ltd and was migrated to Scientific Scholar after the change of Publisher.
Abstract
Female genital tuberculosis (FGTB) is an important cause of infertility in developing countries. Various type of TB salpingitis can be endosalpingitis, exosalpingitis, interstitial TB salpingitis, and salpingitis isthmica nodosa. The fallopian tubes are thickened enlarged and tortuous. Unilateral or bilateral hydrosalpinx or pyosalpinx may be formed. A new sign python sign is presented in which fallopian tube looks like a blue python on dye testing in FGTB.
Keywords
Fallopian tube
female genital tuberculosis
infertility
laparoscopy
python sign

INTRODUCTION
Female genital tuberculosis (FGTB) is common in developing countries and associated with significant morbidity in the form of menstrual dysfunction, infertility, tubal block, peritubal adhesions, intrauterine adhesions, and perihepatic adhesions.[12]
Fallopian tubes are involved in about 90% of the cases with findings such as congested tubes, tubercles, or caseous nodules on them, peritubal adhesions, and tubal blockage at various levels such as cornual block, mid-tubal block, multiple tubal blocks, or fimbrial block, hydrosalpinx, pyosalpinx, and tubo-ovarian masses.[23]
A new sign demonstrated on laparoscopy in a case of FGTB is presented.
CASE REPORT
A 25-year-old woman with family history of pulmonary TB was presented to the Gynecology outpatient department with primary infertility and oligomenorrhea of 3 years. On examination, she was moderately built with body mass index of 23.2 kg/m2. Heart, chest, and abdominal examination were normal. Speculum examination revealed healthy cervix and vagina. Vaginal examination demonstrated anteverted uterus with fullness and induration in both fornices. On investigations, complete hemogram and chest X-ray were normal; Mantoux test was positive. Hysterosalpingogram which was already performed by the referring doctor for infertility before diagnosis of FGTB was made showed bilateral tubal block. Endometrial aspirate performed in premenstrual phase showed positive polymerase chain reaction based on the amplification of the 240 bp region of the MPT 64 gene using primers MPT 1 (59-TCCGCTGCCAGTCGTCTTCC-39; nt 460–479) and MPT 2 (59-GTCCTCGCGAG TCTAGGCCA-39; nt 700–681) with equipment using Amplitron thermocycler (Barnstead/Thermolyne), it also tested positive for culture for mycobacterium tuberculosis using Mycobacterium Growth Indicator Tube-960. Histopathology demonstrated secretory endometrium with no epithelioid granulomas. On diagnostic laparoscopy, there were findings of TB in the pelvis in the form of multiple tubercles on tubes and uterus, bilateral hydrosalpinx with beading of tubes, and few caseous nodules. When methylene blue dye was injected in the uterus, the fallopian tubes became distended and blue colored with beading looking with alternate constrictions and dilatation looking-like “blue pythons” [Figure 1]. Diagnosis of genital TB was made, and she was started on anti-TB therapy. Her postoperative period and follow-up were uneventful.
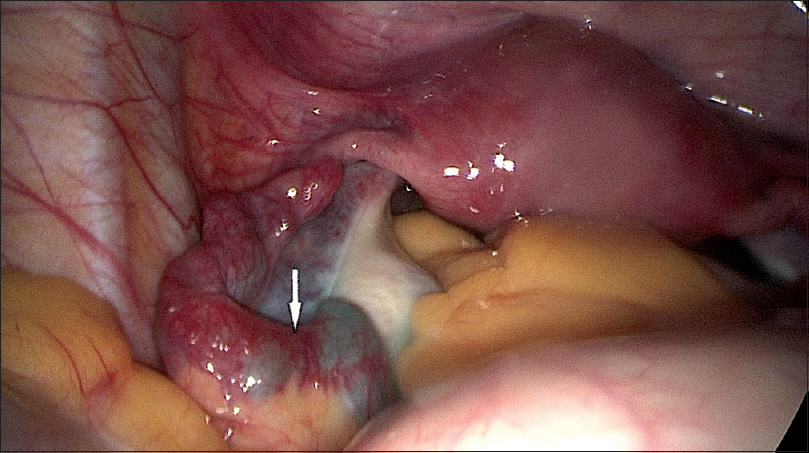
- Left fallopian tube with distension, multiple ballooning, and blue coloration with fimbrial block showing “blue python sign”
DISCUSSION
Being a paucibacillary disease, diagnosis of FGTB may be difficult.[23] Although gold standard in diagnosis of FGTB is demonstration of mycobacterium tuberculosis either on microscopy or culture of endometrial biopsy or presence of epithelioid granuloma on histopathology, they are positive in only few cases leading on to missing of diagnosis in many cases.[23] Polymerase chain reaction on endometrial biopsy is a sensitive and rapid method for detecting mycobacterium DNA (MPT 64 gene) but can be false positive and may not be able to differentiate between infection and disease.[4]
Gene Xpert has recently been introduced in both pulmonary and extra-pulmonary TB as a sensitive and specific method, but its data in FGTB are very sparse.[5]
Imaging modalities such as ultrasound, computed tomography scan, magnetic resonance imaging, and positron emission tomography scan have main role in tubo-ovarian masses.[2] Hysterosalpingography is generally avoided in a suspected case of FGTB due to risk of flare up of the disease but may demonstrate tubal block and other tubal patterns, especially in advanced case.[6]
Hysteroscopy is useful in endometrial disease and may show pale looking endometrium with endometrial cavity being partially or completely obliterated by adhesions of varying grade (Asherman's Syndrome) which may involve ostia.[7] However, laparoscopy is the most reliable tool to diagnose FGTB, especially for tubal, ovarian, and peritoneal disease.[8] There can be tubercles on peritoneum or tubes, tubo-ovarian masses, caseous nodules, encysted ascites, various grades of pelvic adhesions, hydrosalpinx, pyosalpinx, beaded tubes, tobacco pouch appearance, and inability to see tubes due to adhesions.[8] Other authors have also found laparoscopy very useful in diagnosis and management of genital and peritoneal TB with the advantage of avoidance of laparoscopy which is more traumatic and hazardous especially in a case of abdominopelvic TB.[910]
In a case of FGTB, there may a one or more blocks at various levels of fallopian tubes. If there is no cornual block, there is a partial or complete fimbrial block with multiple blocks at various parts of tube as is typical of FGTB, dye enters the tube but remains in various parts of tubes with alternate dilatation and constriction making the tube look like a “blue python” as happened in the present case. The new sign case is easily diagnosed by gynecologists during routine laparotomy performed for infertility patients with suspected FGTB and can aid in its diagnosis.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Acknowledgment
The author is thankful to Dr. Urvashi Singh, Department of Microbiology, for carrying out polymerase chain reaction. The author is also thankful to Prof Alka Kriplani, Prof Sunesh Kumar, Sona Dharmendra and Pawan Kumar for their help.
REFERENCES
- World Health Organization. Global Tuberculosis Control. A Short Update to the 2009 Report. WHO/HTM/TB/2009426. Geneva: WHO; 2009.
- [Google Scholar]
- Tuberculosis and obstetrics and gynaecological practice. In: Studd J, Tan SL, Chervenak FA, eds. Progress in Obstetrics and Gynaecology. Vol 18. Philadelphia: Elsevier; 2008. p. :395-427.
- [Google Scholar]
- Improved diagnostic value of PCR in the diagnosis of female genital tuberculosis leading to infertility. J Med Microbiol. 2005;54(Pt 10):927-31.
- [Google Scholar]
- Xpert MTB/RIF: A new pillar in diagnosis of extrapulmonary tuberculosis? J Clin Microbiol. 2011;49:2540-5.
- [Google Scholar]
- Hysterosalpingographic findings in infertile women with genital tuberculosis. Int J Gynecol Obstet. 2008;101:150-5.
- [Google Scholar]
- Hysteroscopic findings in women with primary and secondary infertility due to genital tuberculosis. Int J Gynecol Obstet. 2009;104:49-52.
- [Google Scholar]
- Laparoscopic findings in female genital tuberculosis. Arch Gynecol Obstet. 2008;278:359-64.
- [Google Scholar]
- Female genital tuberculosis: Early diagnosis by laparoscopy and endometrial polymerase chain reaction. Int J Tuberc Lung Dis. 2010;14:1629-34.
- [Google Scholar]
- Genital and peritoneal tuberculosis: Potential role of laparoscopy in diagnosis and management. J Am Assoc Gynecol Laparosc. 2004;11:269-72.
- [Google Scholar]



