
Translate this page into:
Evaluation of cyclooxygenase-2, P53, vascular endothelial growth factor, and nitric oxide synthase-2 in angiogenesis and growth of tobacco-related malignancies
*Corresponding author: Zeeba S. Jairajpuri, MD, Department of Pathology, Hamdard Institute of Medical Sciences and Research, Hamdard Nagar, New Delhi 110062, India jairajpurizs@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Gautam S, Sangma M, Rana S, Khetrapal S, Kapur S, Jairajpuri ZS. Evaluation of cyclooxygenase-2, P53, vascular endothelial growth factor, and nitric oxide synthase-2 in angiogenesis and growth of tobacco-related malignancies. J Lab Physicians. 2024;16:44-51. doi: 10.1055/s-0043-1772680
Abstract
Objectives:
In India, tobacco consumption is responsible for half of all the cancers in men and a quarter in women. The present study focuses on the expression of cyclooxygenase-2 (COX-2), P53, vascular endothelial growth factor (VEGF), and nitric oxide synthase (NOS) and their relationship with the growth and angiogenesis of tobacco-related malignancies of the oral cavity, esophagus, lungs, and stomach. It further evaluates the carcinogenic action of nicotine and examines whether COX-2 and NOS-2 overexpression is responsible for tumor growth and associated angiogenic VEGF expression via its receptor.
Materials and Methods:
A cross-sectional study on 140 biopsies, resected specimens of cancer of oral cavity, esophagus, stomach, and lungs, was done. Immunohistochemical evaluation for p53, COX-2, VEGF, and inducible NOS was done. Relevant statistical analysis was applied for the significance of the findings.
Statistical Analysis:
Relevant statistical analysis was done using SPSS, chi-square and Fisher's exact tests were applied for the significance of the findings. A p-value of < 0.05 was considered as significant value.
Results:
Immunohistochemical evaluation of pattern of expression of COX-2, NOS-2, VEGF, and p53 was done in both tobacco- and nontobacco-associated cases. The results of the present study revealed an upregulation of COX-2, NOS-2, VEGF, and p53 in all the malignancies.
Conclusion:
The present results indicated that p53 protein accumulation and increased expression of COX-2, NOS-2, and VEGF might be responsible for carcinogenesis and tumor aggressiveness by enhancing angiogenesis. A possible significant effect of nicotine on COX-2 and P53 expression in tumorigenesis is revealed. These data might have important implications for the therapeutic use of COX-2, NOS-2, and VEGF inhibitors as well as of p53 gene therapy in future anticancer therapeutic strategies in tobacco-related malignancies.
Keywords
tobacco
malignancy
angiogenesis

INTRODUCTION
Cancers are known to be influenced by environmental factors and genetic disorders that play an important role in the pathogenesis of human cancers. With this regard, consumption and exposure to tobacco smoke is a major public health issue.[1] In India, tobacco consumption is responsible for half of all the cancers in men and a quarter of all cancers in women. Proportion of tobacco-related cancers out of all cancers is high in India with the Northeast region being at the highest risk among all cancer registries in India. Esophagus, lung, hypopharynx, and mouth along with stomach, were the leading cancer sites for both men and women.[2]
Cyclooxygenase enzyme (COX) catalyzes the formation of eicosanoids including prostaglandins from arachidonic acid. There are two distinct isoforms of COX, COX-1 and COX-2. COX-1 is constitutively expressed in most mammalian tissues. COX-2 plays an important role in cancer development through catalyzing the biogenesis of inflammation-promoting prostaglandins.[3] It is induced by inflammation, growth factor, tumor promoters, oncogenes, and carcinogens. Normally, COX-2 proteins are either undetectable or expressed only at low levels in most tissues. COX-2 is overexpressed in transformed cells and cancers of the oral cavity, lungs, and the gastrointestinal tract and is thought to be a proliferative marker.[4,5]
The tumor suppressor gene p53 is the most common target for genetic alteration in cancers. p53 protein functions as a critical gatekeeper against the formation of cancer that prevents the propagation of genetically damaged cells. Mutation of this gene predisposes to the multistep process of carcinogenesis and the expression of p53 has been found to be higher in tobacco-related malignancies.[6,7]
Angiogenesis is known to play a central role in the growth and metastasis of malignant disease, regulated by pro and inhibitory angiogenic growth factors. The proangiogenic growth factors include vascular endothelial growth factor (VEGF).[8] There is accumulating evidence that high VEGF expression plays an important role in the pathogenesis of solid tumors.[9,10]
Nitric oxide Synthase (NOS) is expressed in macrophages and various other cells, including various tumor cells where a positive correlation between inducible NOS (iNOS) expression and tumor progression has been extensively reported.[11]
The present study focuses on the expression of COX-2, P53, VEGF, and NOS and their relationship with the growth and angiogenesis of tobacco-related malignancies of the oral cavity, esophagus, lungs, and stomach. It further evaluates the carcinogenic action of nicotine and examines whether COX-2 and NOS-2 overexpression is responsible for tumor growth and tumor-associated angiogenic VEGF expression via its receptor.
MATERIAL AND METHODS
The present cross-sectional study was conducted in a tertiary care hospital and its affiliated institute, on biopsies and resected specimens received from patients with cancer of oral cavity, esophagus, stomach, and lungs, presenting at the department of medicine and surgery over a period of 3 years. A total of 140 cases were included in the study. Clinical details were obtained from the medical records of the patients. A total of 120 patients had history of tobacco usage while 20 biopsies were from patients with no history of tobacco intake and were included as controls. Formalin-fixed samples were processed and embedded for preparing paraffin sections. Serial tissue sections were stained with hematoxylin and eosin for histopathological diagnosis and classification of these malignancies. Broder’s classification was followed for cancer of oral cavity, Laurens classification for gastric cancer, and the World Health Organization classification for both esophagus and lung cancer. Grading was done as recommended by the American Joint Committee on Cancer. Clinical data including age, gender, and symptoms of disease were also noted.
Immunohistochemical evaluation of the tissue was done, sections were obtained on poly-L-lysine-coated slides and were subjected to immunohistochemical staining using mono-/polyclonal antibodies by labeled streptavidin– biotin method using diaminobenzidine as substrate which appears as a brown granule at site of antigen antibody reaction. Specific staining for each protein was categorized as either positive or negative based on the presence of brown color staining. More than 10% cells positively stained were graded as positive. Clear staining for nuclei (p53; Dako, 1:50 dilution), cytoplasm, and cell membrane (COX-2; Santacruz, 1:50 dilution, VEGF; BD Biosciences,1:50 dilution, and iNOS; Laboratory Vision, 1:50 dilution) was the criterion for a positive reaction. Relevant statistical analysis was done using SPSS, chi-square and Fisher’s exact tests were applied for the significance of the findings. A p-value of < 0.05 was considered as significant value.
RESULTS
A total of 140 cases were included in the study. Thirty (30) cases each from the lesions of oral cavity, esophagus, gastric, and lungs, with history of tobacco intake, were studied and compared with controls (patients with no history of tobacco intake), five from each of these sites (Table 1). Analysis of the cases showed a predominance of male patients comprising of 105 out of 140 (75%) cases, 120 cases were tobacco users of which 99 (82.5%) were males; however, a female preponderance (70%) was seen in nontobacco users. The male-to-female (M:F) ratio in the study cases was 5:1, whereas in the controls the ratio was reversed with M: F = 0.4:1. The peak incidence of the malignancies associated with chronic tobacco intake was seen in the 4th to 6th decades while nontobacco-associated malignancies was seen most prevalent in the 5th to 7th decades. Majority of the cases were in the 51 to 60 years age group.
| Site of malignancy | Histological diagnosis | Tobacco users (n = 120) | Nontobacco users (n = 20) |
|---|---|---|---|
| Oral cavity (n = 35) | Well differentiated SCC | 11 | 2 |
| Moderately differentiated SCC | 10 | 2 | |
| Poorly differentiated SCC | 9 | 1 | |
| Esophagus (n = 35) | Well differentiated SCC | 12 | 2 |
| Moderately differentiated SCC | 10 | 1 | |
| Poorly differentiated SCC | 8 | 2 | |
| Stomach (n = 35) | Intestinal | 15 | 3 |
| Diffuse | 15 | 2 | |
| Lung (n = 35) | Well differentiated SCC | 10 | 2 |
| Moderately differentiated SCC | 6 | 2 | |
| Poorly differentiated SCC | 9 | 1 | |
| Small cell carcinoma | 5 | 0 |
SCC, squamous cell carcinoma.
The predominant tumor histology in the study was that of squamous cell carcinoma (SCC) (71.5%) while adenocarcinoma and small cell carcinoma constituted 25 and 3.5% of the study group, respectively (Figure 1).
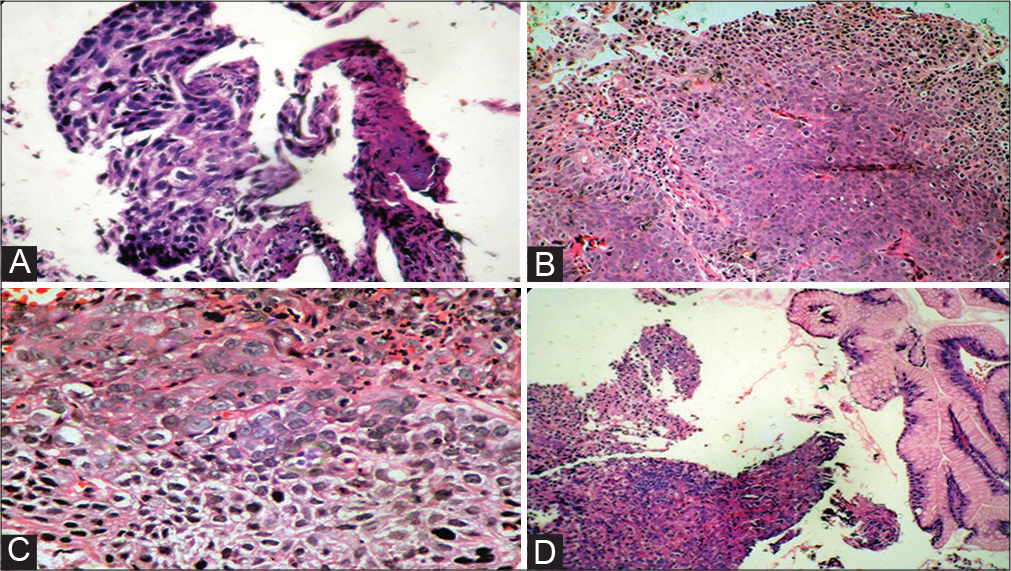
- (A) Hematoxylin and eosin (H&E) photomicrograph of poorly differentiated squamous cell carcinoma (SCC) of lung (40 × ). (B) H&E photomicrograph exhibiting moderately differentiated SCC of lungs. (C) H&E stained photomicrograph exhibiting poorly differentiated SCC of esophagus. (D) H&E photomicrograph of gastric adenocarcinoma.
Immunohistochemical evaluation of pattern of expression of all four markers was done in both tobacco and nontobacco-associated cases. The percent positivity was evaluated (Table 2) and compared with controls.
| Markers | Tobacco associated, n = 30 (% positivity) | Nontobacco associated, n = 5 (% positivity) |
|---|---|---|
| Oral cavity | ||
| p53 | 21 (70) | 3 (60) |
| COX-2 | 22 (73.3) | 2 (40) |
| NOS-2 | 13 (43.3) | 2 (40) |
| VEGF | 22 (73.3) | 3 (60) |
| Esophagus | ||
| p53 | 22 (73.3) | 2 (40) |
| COX-2 | 23 (76.6) | 2 (40) |
| NOS-2 | 16 (53.3) | 2 (40) |
| VEGF | 24 (80) | 3 (60) |
| Lungs | ||
| p53 | 17 (56.6) | 2 (40) |
| COX-2 | 16 (53.3) | 3 (60) |
| NOS-2 | 13 (43.3) | 2 (40) |
| VEGF | 18 (60) | 3 (60) |
| Stomach | ||
| p53 | 22 (73.3) | 3 (60) |
| COX-2 | 17 (56.6) | 2 (40) |
| NOS-2 | 15 (50) | 2 (40) |
| VEGF | 23 (76.6) | 3 (60) |
COX-2, cyclooxygenase-2; NOS-2, nitric oxide synthase-2; VEGF, vascular endothelial growth factor.
As is evident from the tabulated results, an upregulation of each marker was seen in all malignancies. It was seen that the activity of COX-2 and p53 was particularly increased in tobacco-related malignancies of the oral cavity and esophagus.
The expression of COX-2 was seen to be significantly higher in malignancies of both oral cavity (p = 0.018) and esophagus (p = 0.008) associated with chronic tobacco use as compared with those with no history of tobacco intake (Figure 2). Comparison of p53 between the two groups did not show any significant difference in cancers of the oral cavity, lung, and stomach, while a significant difference was seen in the expression of p53 (p = 0.018) in esophageal carcinoma. More so, the expression of COX-2 in lung and gastric carcinoma did not show any significant difference (p > 0.05) in both the cases and controls. NOS-2 and VEGF did not show any significant difference (> 0.05) in their expression in cases as well as controls in oral cavity, esophagus, both SCC and small cell carcinoma lung, as well as gastric adenocarcinoma.
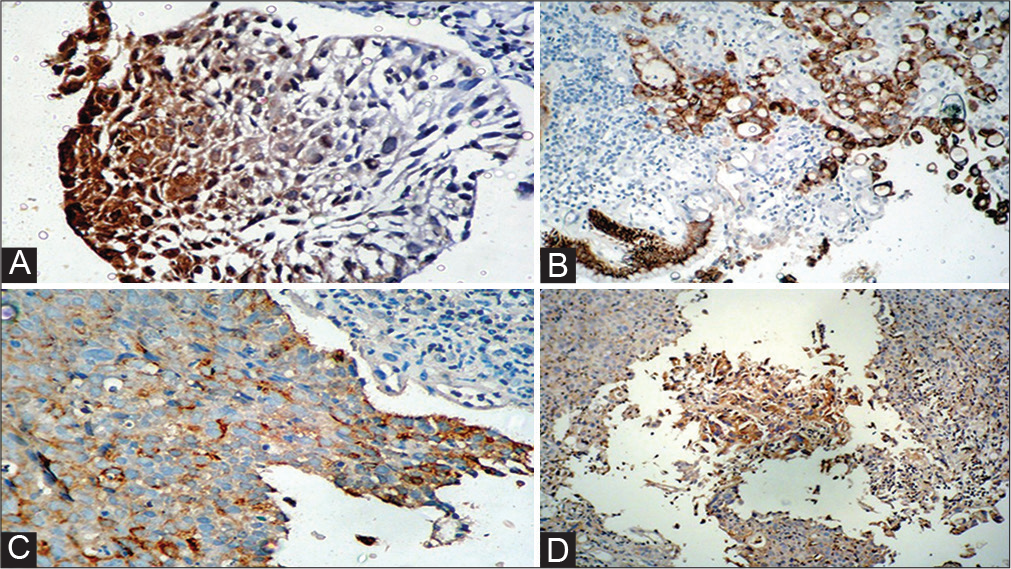
- (A) Photomicrograph of poorly differentiated squamous cell carcinoma (SCC) of esophagus showing cytoplasmic positivity for cyclooxygenase-2 (COX-2). (B) Photomicrograph of gastric adenocarcinoma exhibiting cytoplasmic positivity for COX. (C) Photomicrograph of poorly differentiated SCC of lung exhibiting cytoplasmic positivity for COX-2. (D) Photomicrograph of poorly differentiated SCC of esophagus showing cytoplasmic positivity for COX-2.
We also analyzed the expression of the four markers in the tobacco-related malignancies according to the differentiation of the lesions (Table 3). The expression of COX-2 was seen to be significantly higher in moderately and poorly differentiated SCC of the oral cavity (p < 0.05) as compared with well-differentiated SCC. However, the expression of other markers, that is, p53, NOS-2, and VEGF did not show any statistical significance (p > 0.05) in relation to the differentiation of the tumor (Figure 3). On the other hand, in cases of esophageal and lung carcinoma including small cell carcinoma, no significant difference was seen in the expression of p53, COX-2, NOS-2, and VEGF in relation to the degree of differentiation of the tumors. In cases of gastric adenocarcinoma, no significant difference (p > 0.05) was seen in the expression of all the four markers between diffuse and intestinal type of adenocarcinoma.
| Histological grade of malignancy | No. ofsamples | COX-2 (%) | p53 (%) | NOS-2 (%) | VEGF (%) |
|---|---|---|---|---|---|
| Oral cavity SCC | |||||
| Well differentiated | 11 | 06 (54.5) | 07 (63.6) | 04 (36.3) | 07 (63.6) |
| Moderately differentiated | 10 | 09 (90) | 06 (60) | 05 (50) | 07 (70) |
| Poorly differentiated | 09 | 07 (77.7) | 08 (88.8) | 04 (44.4) | 08 (88.8) |
| Total | 30 | 22 | 21 | 13 | 22 |
| p-value 0.02 (moderately differentiated SCC)0.05 (poorly differentiated SCC) | p-value > 0.05 | p-value > 0.05 | p-value > 0.05 | ||
| Esophagus SCC | |||||
| Well differentiated | 12 | 08 (66.6) | 09 (75) | 05 (41.6) | 10 (83.3) |
| Moderately differentiated | 10 | 08 (80) | 07 (70) | 05 (50) | 07 (70) |
| Poorly differentiated | 08 | 07 (87.5) | 06 (75) | 06 (75) | 07 (87.5) |
| Total | 30 | 23 | 22 | 16 | 24 |
| p-value = 0.008 | p-value = 0.018 | p-value > 0.05 | p-value > 0.05 | ||
| Lung (SCC and small cellcarcinoma) | |||||
| Well differentiated | 10 | 05 (50) | 05 (50) | 04 (40) | 05 (50) |
| Moderately differentiated | 6 | 04 (66.6) | 03 (50) | 02 (33.3) | 04 (66.6) |
| Poorly differentiated | 9 | 05 (55.5) | 06 (66.6) | 05 (55.5) | 06 (66.6) |
| Small cell carcinoma | 5 | 2 (40) | 3 (60) | 2 (40) | 3 (60) |
| Total | 30 | 16 | 17 | 13 | 18 |
| p-value > 0.05 | p-value > 0.05 | p-value > 0.05 | p-value > 0.05 | ||
| Gastric adenocarcinoma | |||||
| Diffuse | 15 | 09 (60) | 10 (66.6) | 7 (46.6) | 11 (73.3) |
| Intestinal | 15 | 08 (53.3) | 12 (80) | 08 (53.3) | 12 (80) |
| Total | 30 | 17 | 22 | 15 | 23 |
| p-value > 0.05 | p-value > 0.05 | p-value > 0.05 | p-value > 0.05 |
COX-2, cyclooxygenase-2; NOS-2, nitric oxide synthase-2; SCC, squamous cell carcinoma; VEGF, vascular endothelial growth factor.
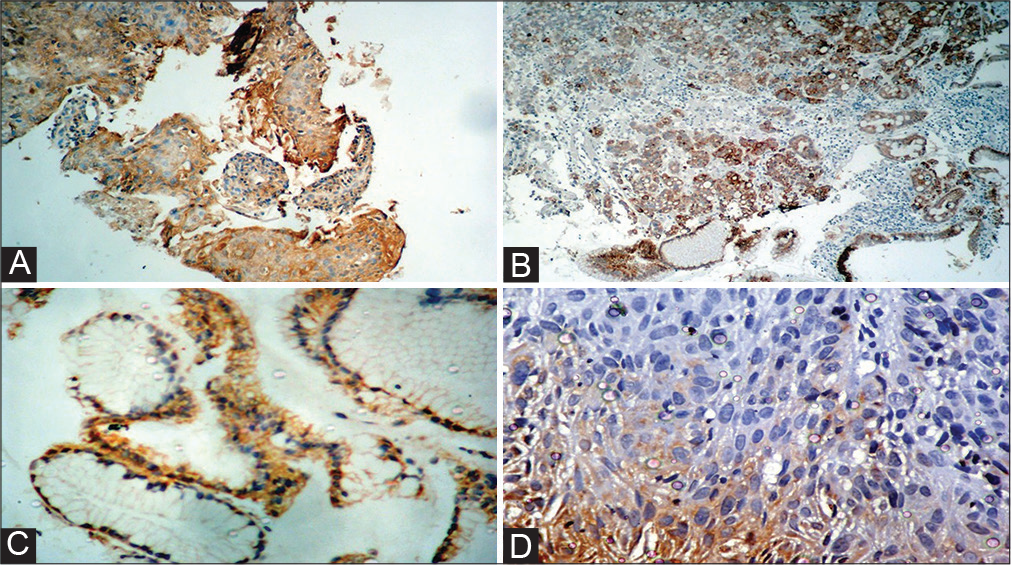
- (A) Photomicrograph of gastric adenocarcinoma exhibiting cytoplasmic positivity for vascular endothelial growth factor (VEGF). (B) Photomicrograph of moderately differentiated squamous cell carcinoma (SCC) of lung showing cytoplasmic staining for VEGF. (C) Photomi- crograph of gastric adenocarcinoma showing cytoplasmic positivity for VEGF (40 × ). (D) Photomicrograph of poorly differentiated SCC showing cytoplasmic positivity for nitric oxide synthase-2 (NOS-2).
The overall SCC immunohistochemical profile including 100 cases from the oral cavity, esophagus, and lungs (both tobacco and nontobacco associated) were evaluated (Table 4). All the four markers were overexpressed in the lesions in both the groups.
| Marker profile | Tobacco associated, n = 85 (%) | Nontobacco associated, n = 15 (%) | p-Value |
|---|---|---|---|
| p53 | 57 (67%) | 8 (53.3%) | > 0.05 |
| COX-2 | 59 (69.4%) | 6 (40%) | < 0.05(0.039) |
| NOS-2 | 40 (47%) | 5 (33.3%) | > 0.05 |
| VEGF | 61 (71.7%) | 8 (53.3%) | > 0.05 |
COX-2, cyclooxygenase-2; NOS-2, nitric oxide synthase-2; SCC, squamous cell carcinoma; VEGF, vascular endothelial growth factor.
The expression of COX-2 was found to be significantly higher (p = 0.039) in SCCs associated with tobacco intake as compared with the controls. However, there was no significant difference (p > 0.05) in the expression of the other markers, that is, p53, NOS-2, and VEGF in both the cases and controls.
On comparing the immunohistochemical profile of all SCC and gastric adenocarcinoma cases, no significant difference (p = 0.05) in the expression of the markers (i.e., p53, COX-2, NOS-2, and VEGF), (Figure 4) between SCC and adenocarcinoma associated with tobacco intake was seen, although overexpression of the markers were seen in all the cases (Table 5).
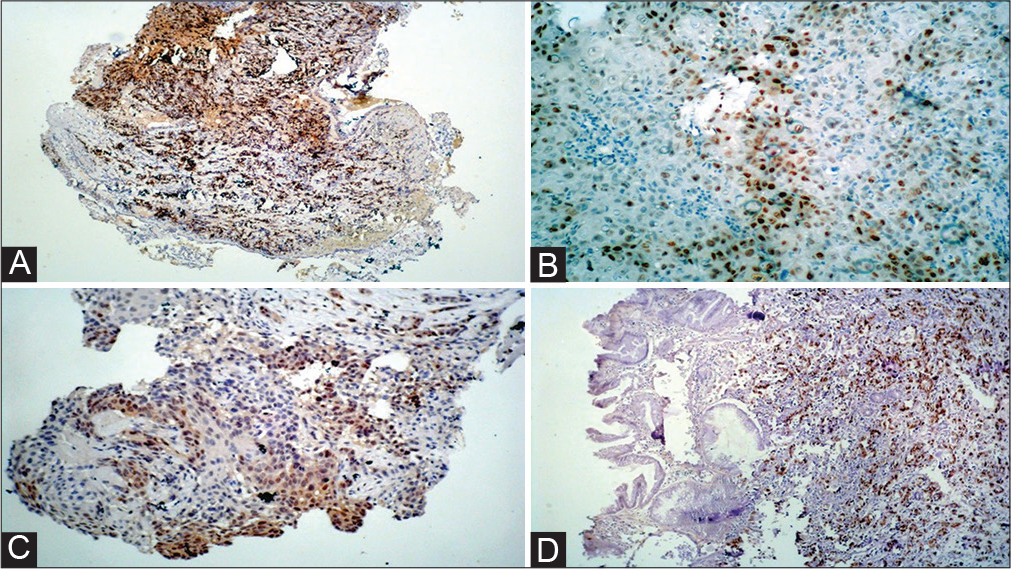
- (A) Photomicrograph of small cell lung carcinoma exhibiting nuclear positivity for p53. (B) Photomicrograph of moderately differentiated squamous cell carcinoma (SCC) of esophagus exhibiting nuclear positivity for p53. (C) Photomicrograph of gastric adenocarcinoma exhibiting nuclear positivity for p53. (D) Photomicrograph of moderately differentiated SCC of lung exhibiting nuclear positivity for p53.
| Marker profile | SCC, n = 85 (%) |
Adenocarcinoma, n = 30 (%) |
p-Value |
|---|---|---|---|
| p53 | 57 (67) | 22 (73.3) | > 0.05 |
| COX-2 | 59 (69.4) | 17 (56.6) | |
| NOS-2 | 40 (47) | 15 (50) | |
| VEGF | 61 (71.7) | 23 (76.6) |
COX-2, cyclooxygenase-2; NOS-2, nitric oxide synthase-2; SCC, squamous cell carcinoma; VEGF, vascular endothelial growth factor.
DISCUSSION
Epidemiologic data have strongly linked tobacco intake in various forms (cigarette smoking, chewing pan, etc.) to the development of certain cancers. Repeated exposure to specific carcinogens in cigarette smoke may cause multiple neoplastic lesions in the mucosa of the aerodigestive tract.[12]
The upper aerodigestive tract is the only area in the body in which the alimentary tract and the airways form a common conduit and is an ideal site for evaluating the independent and synergistic effects of tobacco. Tumorigenesis due to tobacco use has been associated with mutations of p53 gene, disruption of cell-cycle control, activation of oncogenes, and inactivation of several tumor suppressor genes.[13,14]
COX-2 is an essential enzyme in the biogenesis of inflammation-promoting prostaglandins. Overexpression of COX-2 has been identified in many solid tumors and premalignant lesions, including oral cancers and oral premalignant lesions.[15] COX-2 has been explored because it is thought to play an important role in the initiation and progression of carcinomas of various organs. Enhanced synthesis of prostaglandins, results from upregulation of COX-2, increases the proliferative activity of neoplastic cells, cancer invasiveness and metastasis, promotes angiogenesis, as well as inhibits apoptosis.[16,17] We have established through this study that deregulation of COX-2 gene expression occurs in malignant tissues. This upregulation of COX-2 in malignant cells predisposes the cells to further deregulation of several progression-related gene expression markers. Further, the expression of COX-2 in both tobacco-and nontobacco-related malignancies showed a significant increase in the expression of COX-2 in tobacco-related malignancies as compared with the nontobacco-related cases in both the oral cavity and the esophagus (p = 0.018 and p = 0.008, respectively). The expression was also seen to be increased in moderately and poorly differentiated SCC of the oral cavity when compared with well-differentiated SCC (p = 0.02 and 0.05, respectively). Banerjee et al established through their study that deregulation of COX-2 gene expression occurs in early dysplastic oral tissues.[18] Gallo et al also found similar results in cases of head and neck SCC.[19] Upregulation of COX-2 has also been reported in malignant tissues as compared with normal oral tissues.[20]
In malignancies of the lung and stomach, although an overexpression of COX-2 was seen in this study, no significant difference was seen in the expression of the protein in both tobacco- and nontobacco-related cases. Further, in this study, there was no significant preference seen in the expression of the protein with regard to the histological grading of the tumors in the esophagus, lungs, and stomach. A nonsignificant association between COX-2 expression and tobacco use has been reported by other authors.[21,22] However, increased expression of COX-2 did not show a preference to any histological subtypes of tumor.[22] Overexpression of COX-2 might contribute to angiogenesis and growth of gastric cancer.[23]
All the malignancies studied showed overexpression of p53. The expression of p53 was found to be higher in tobacco-related malignancies of the esophagus as compared with nontobacco-related esophageal malignancies (p = 0.018). Overexpression of p53 in association with cigarette smoking may play a critical role in esophageal SCC carcinogenesis among high-risk population. Furthermore, the presence of abnormally accumulated p53 in the morphologically normal tissue adjacent to the resected tumor may be a predictor of future recurrence of tumor.[24] Overexpression of p53 staining did not show any correlation with tumor grading in all the malignancies in the present study. However, a significant difference in p53 expression among grades of epithelial dysplasia has been reported by Shetty et al, suggesting that p53 may play a more predictive role in assessing the changes among precancerous lesions.[25]
Malignancies of the lung showed expression of p53 in 56% of SCCs and 60% of small cell lung cancer. There was no significant correlation that was seen in between the tobacco-and nontobacco-related cases and between the various tumor grades. Exposure to tobacco is known to produce genomic mutations in lung cancer, including mutation of the tumor suppressor p53, alterations of which are very frequent in SCC, adenocarcinoma, and small cell carcinoma of the lung. The critical role of p53 alteration is in malignant transformation, histologic progression, invasion, and metastasis.[26]
In this study, p53 was expressed in 73.3% of gastric adenocarcinomas associated with tobacco intake and in 60% of nontobacco-related adenocarcinomas. However, there was no significant correlation in the expression of p53 with regard to tumor differentiation. These findings were coherent with a study conducted by Padma Malini et al[27] who also concluded that p53 expression was seen in younger population, increased depth of invasion, and lymph node metastasis, hence indicating that p53 is a prognostic indicator for gastric malignancies.[27,28] Detecting p53 expression in patients with gastric cancer may aid in deciding the intensity of the therapies. Therapy modalities intending to regulate p53 expression and activators may be a hope for gastric cancer, known as a progressive disease.[28]
Angiogenesis, the process of new vessel development, is one of the critical steps in tumor growth, being involved not only in local extension but also being responsible for metastasis. Angiogenesis is activated early in carcinogenesis due to an imbalance between positive and negative angiogenic factors produced by both tumor cells and normal cells.[29]
In the present study, VEGF, the angiogenic marker, was found to be expressed in all the malignancies evaluated. However, positivity of VEGF did not show any correlation with tumor grading in all the cases. VEGF plays an important role in tumor progression, its overexpression correlates with a bad prognosis, and may improve high-risk patient selection, and these patients may obtain additional survival benefits if treated more aggressively.[29] An increased expression of VEGF in the oral cavity was seen in tobacco-related malignancies in the present study. The expression of VEGF is increased in the processes of oral SCC (OSCC), progression, and proliferation. VEGF is connected to lymph node metas-tasis in OSCC.[30] In SCCs of the esophagus, VEGF expression was seen in 80% cases of tobacco-related malignancies in our study. High VEGF levels are significantly associated with well-differentiated tumors, advanced stage (depth of invasion and blood vessel invasion), high incidence of distant metastases after surgery, and poorer prognosis.[31] Gastric adenocarcinomas also showed increased expression of VEGF in the tobacco-associated malignancies in the present study, although no significant correlation was observed in the intestinal and diffuse-type gastric cancer. The results of the presented research suggest a significant role of VEGF and CXCR4 in the biology of gastric cancer. The possible predictive value of both proteins may be promising. Nevertheless, further analyses are required to assess their usefulness in clinical practice. Identifying specific biomarkers for the metastatic potential of primary gastric cancer would allow better patient selection for more radical treatment.[29] Positive association was seen with high vascular grade in the current study although no difference was seen in tobacco and nontobacco cases. Expert opinion is VEGF plays an important role in sustaining the development and progression of lung cancer and it might represent an attractive target for therapeutic strategies. To improve the efficacy of anti-VEGF therapies in lung cancer, potential strategies might be the employment of combinatory therapies with immune checkpoint inhibitors or agents that inhibit signaling pathways and proangiogenic factors activated in response to VEGF blockade, and the identification of novel targets in the VEGF cascade.[32]
In this study, NOS-2 was seen to be expressed in tobacco-related and nontobacco-related malignancies of the oral cavity. However, immunoreactivity of NOS-2 was not significantly different in tobacco- and nontobacco-related malignancies of the oral cavity, esophagus, lung, and gastric adenocarcinomas. NOS activity has been detected in tumor cells of various histogenetic origins and has been associated with tumor grade, proliferation rate, and expression of important signaling components associated with cancer development. It appears that high levels of NOS expression (for example, generated by activated macrophages) may be cytostatic or cytotoxic for tumor cells, whereas low level activity can have the opposite effect and promote tumor growth. Paradoxically, therefore, NO (and related reactive nitrogen species) may have both genotoxic and angiogenic properties. Increased NO generation in a cell may select mutant p53 cells and contribute to tumor angiogenesis by upregulating VEGF. Furthermore, NOS/NO levels are often associated with increased metastasis, leading to poor patient prognosis. The association of elevated NOS-2 expression with cancers arising due to bacterial, viral, and fungal infections suggests an important relationship of the same with tumor immune response and chronic inflammation.[33]
CONCLUSIONS
The results of the present research reveal an upregulation of COX-2, NOS-2, VEGF, and p53 in all the malignancies. It was seen that the activity of COX-2 and p53 was particularly increased in tobacco-related malignancies of the oral cavity and esophagus. This reveals a possible significant effect of nicotine on COX-2 and P53 expression in tumorigenesis. The present results also indicated that p53 protein accumulation and increased expression of COX-2, NOS-2, and VEGF might be responsible for carcinogenesis and tumor aggressiveness by enhancing angiogenesis. Further, investigations will be required to determine the exact role of p53, COX-2, NOS-2, and VEGF in tobacco-related human carcinogenesis as well as the mechanism(s) by which the most frequently mutated tumor suppressor gene and pathways are involved in the regulation of several biological functions in human cancers, including inflammatory reactions, proliferation, apoptosis, and neoangiogenesis. These data might have important implications for the therapeutic use of COX-2, NOS-2, and VEGF inhibitors as well as of p53 gene therapy in future anticancer therapeutic strategies in tobacco-related malignancies.
Conflict of interest
None declared.
References
- The molecular mechanisms of tobacco in cancer pathogenesis. Int J Cancer Manag. 2017;10:e7902.
- [CrossRef] [Google Scholar]
- Tobacco-related cancers in India: a review of incidence reported from population-based cancer registries. Indian J Med Paediatr Oncol. 2016;37:152-157.
- [CrossRef] [PubMed] [Google Scholar]
- Cyclooxygenase-2 gene polymorphisms reduce the risk of oral premalignant lesions. Cancer. 2009;115:1498-1506.
- [CrossRef] [PubMed] [Google Scholar]
- Areca nut extract up-regulates prostaglandin production, cyclooxygenase-2 mRNA and protein expression of human oral keratinocytes. Carcinogenesis. 2000;21:1365-1370.
- [CrossRef] [PubMed] [Google Scholar]
- Overexpression of COX-2 gene in oral cancer is independent of stage of disease and degree of differentiation. Int J Oral Maxillofac Surg. 2008;37:379-383.
- [CrossRef] [PubMed] [Google Scholar]
- Overexpression of p53 protein in betel-and tobacco-related human oral dysplasia and squamous-cell carcinoma in India. Int J Cancer. 1994;58:340-345.
- [CrossRef] [PubMed] [Google Scholar]
- Uncovering the role of p53 splice variants in human malignancy: a clinical perspective. OncoTargets Ther. 2013;7:57-68.
- [CrossRef] [PubMed] [Google Scholar]
- Angiogenesis and non-small cell lung cancer. Lung Cancer. 2000;27:81-100.
- [CrossRef] [PubMed] [Google Scholar]
- Association of vascular endothelial growth factor expression with intratumoral microvessel density and tumour cell proliferation in human epidermoid lung carcinoma. Br J Cancer. 1996;73:931-934.
- [CrossRef] [PubMed] [Google Scholar]
- Prognostic value of ERBB-1, VEGF, cyclin A, FOS, JUN and MYC in patients with squamous cell lung carcinomas. Br J Cancer. 1998;77:663-669.
- [CrossRef] [PubMed] [Google Scholar]
- Modulation of prostaglandin biosynthesis by nitric oxide and nitric oxide donors. Pharmacol Rev. 2005;57:217-252.
- [CrossRef] [PubMed] [Google Scholar]
- Association between cigarette smoking and mutation of the p53 gene in squamous-cell carcinoma of the head and neck. N Engl J Med. 1995;332:712-717.
- [CrossRef] [PubMed] [Google Scholar]
- The Health Consequences of Smoking-50 Years of Progress: A Report of the Surgeon General Atlanta, GA: Centers for Disease Control and Prevention (US); 2014.
- [Google Scholar]
- Tobacco smoke carcinogens, DNA damage and p53 mutations in smoking-associated cancers. Oncogene. 2002;21:7435-7451.
- [CrossRef] [PubMed] [Google Scholar]
- Cyclooxygenase-2 expression in oral squamous cell carcinoma. Int J Immunopathol Pharmacol. 2004;17:273-282.
- [CrossRef] [PubMed] [Google Scholar]
- Overexpression of COX-2 in oral squamous cell carcinoma patients undergoing chemoradiotherapy. Natl J Maxillofac Surg. 2011;2:17-21.
- [CrossRef] [PubMed] [Google Scholar]
- Cyclooxygenase-2 and cancer: a silent link with fatal ending. Int J Pathol. 2013;11:32-38.
- [Google Scholar]
- Deregulated cyclooxygenase-2 expression in oral premalignant tissues. Mol Cancer Ther. 2002;1:1265-1271.
- [Google Scholar]
- Down-regulation of nitric oxide synthase-2 and cyclooxygenase-2 pathways by p53 in squamous cell carcinoma. Am J Pathol. 2003;163:723-732.
- [CrossRef] [PubMed] [Google Scholar]
- Mechanisms of oral carcinogenesis induced by dibenzo[a,l]pyrene: an environmental pollutant and a tobacco smoke constituent. Int J Cancer. 2013;133:1300-1309.
- [CrossRef] [PubMed] [Google Scholar]
- TP53 and KRAS mutation load and types in lung cancers in relation to tobacco smoke: distinct patterns in never, former, and current smokers. Cancer Res. 2005;65:5076-5083.
- [CrossRef] [PubMed] [Google Scholar]
- Nitric oxide synthase, cyclooxygenase 2, and vascular endothelial growth factor in the angiogenesis of non-small cell lung carcinoma. Clin Cancer Res. 2000;6:4739-4744.
- [Google Scholar]
- The function and mechanism of COX-2 in angiogenesis of gastric cancer cells. J Exp Clin Cancer Res. 2011;30:13.
- [CrossRef] [PubMed] [Google Scholar]
- Association of p53/p21 expression with cigarette smoking and prognosis in esophageal squamous cell carcinoma patients. World J Gastroenterol. 2010;16:4958-4967.
- [CrossRef] [PubMed] [Google Scholar]
- Assessment and comparison of p53 and p63 expression in oral epithelial dysplasia and squamous cell carcinoma. SRM J Res Dent Sci. 2014;5:149-154.
- [CrossRef] [Google Scholar]
- Smoking, p53 mutation, and lung cancer. Mol Cancer Res. 2014;12:3-13.
- [CrossRef] [PubMed] [Google Scholar]
- Study of expression of P53 in gastric carcinoma-as a prognostic indicator. Int Arch Int Med. 2016;3:54-60.
- [Google Scholar]
- Prognostic significance of p53 in gastric cancer: a meta-analysis. Asian Pac J Cancer Prev. 2015;16:327-332.
- [CrossRef] [PubMed] [Google Scholar]
- The expression and prognostic significance of VEGF and CXCR4 in gastric cancer: correlation with angiogenesis, lymphangiogenesis and progression. Curr Issues Mol Biol. 2022;44:3075-3088.
- [CrossRef] [PubMed] [Google Scholar]
- Vascular Endothelial Growth Factor Expression in the Pathological Angiogenesis in Oral Squamous Cell Carcinoma [Internet] Oral Diseases IntechOpen; 202 0Accessed August 6, 2023 at: http://dx.doi.org/10.5772/intechopen.90924
- [Google Scholar]
- Expression of cyclooxygenase-2, vascular endothelial growth factor, and epidermal growth factor receptor in Chinese patients with esophageal squamous cell carcinoma. J Cancer Res Ther. 2015;11:C44-C48.
- [CrossRef] [PubMed] [Google Scholar]
- VEGF as a potential target in lung cancer. Expert Opin Ther Targets. 2017;21:959-966.
- [CrossRef] [PubMed] [Google Scholar]
- Inducible nitric oxide synthase in the carcinogenesis of gastrointestinal cancers. Antioxid Redox Signal. 2017;26:1059-1077.
- [CrossRef] [PubMed] [Google Scholar]



